Last updated: July 1, 2026
Quick Answer
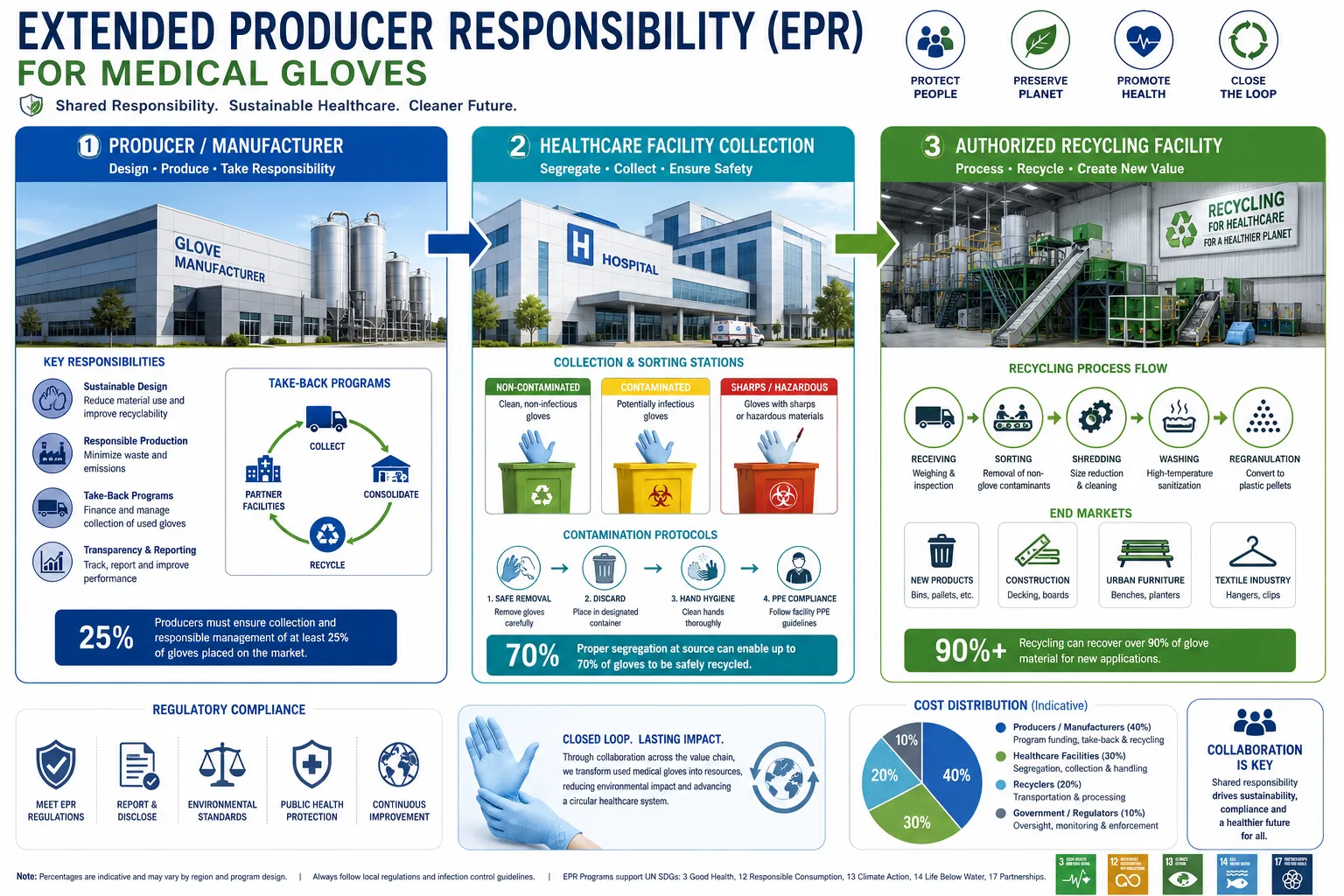
Healthcare facilities worldwide discard an estimated 7.5 million tons of single-use gloves annually, with nitrile gloves comprising the majority. Nitrile Glove Waste Reduction Strategies: Extended Producer Responsibility and Hospital Recycling Programs address this crisis through two complementary approaches: EPR frameworks that shift waste management costs and responsibilities to manufacturers, and hospital-based recycling initiatives that divert used gloves from landfills. These programs can reduce a hospital’s glove waste by 40-60% while cutting disposal costs by 20-35%, though implementation requires careful attention to contamination protocols and regulatory compliance.
Key Takeaways
- Extended Producer Responsibility (EPR) for medical gloves shifts waste management costs from hospitals to manufacturers, creating financial incentives for recyclable product design
- Hospital nitrile glove recycling programs can divert 40-60% of glove waste from landfills when properly implemented with contamination controls
- Non-contaminated nitrile gloves from administrative areas, food service, and non-infectious patient care can be recycled through specialized programs
- EPR regulations for medical gloves are advancing in the EU, with France and Germany leading pilot programs, while US adoption remains voluntary and limited
- Recycling costs hospitals approximately $0.15-0.30 per pound of gloves, compared to $0.08-0.12 for landfill disposal, but total waste management costs often decrease
- Major manufacturers including Kimberly-Clark, Halyard Health, and Cardinal Health now offer take-back programs in select markets
- Common implementation mistakes include mixing contaminated and clean gloves, inadequate staff training, and underestimating collection logistics
- Small clinics with fewer than 50 employees face higher per-unit costs but can join regional consortiums to achieve economies of scale
- Recycled nitrile becomes playground surfaces, athletic tracks, industrial mats, and construction materials after processing
- Contaminated gloves from surgical suites and infectious disease units cannot enter standard recycling streams and require medical waste incineration
What Is Extended Producer Responsibility for Medical Gloves
Extended Producer Responsibility (EPR) for medical gloves is a policy framework that assigns manufacturers legal and financial responsibility for the entire lifecycle of their products, including collection, recycling, and proper disposal after use. Unlike traditional waste management where hospitals and municipalities bear all disposal costs, EPR shifts these obligations upstream to the companies that design and profit from glove sales.
Under EPR systems, glove manufacturers must either establish their own take-back and recycling infrastructure or pay into collective schemes that fund waste management programs. This creates direct financial incentives for companies to design products that are easier to recycle, use less material, or incorporate recycled content.
The European Union has been the global leader in medical glove EPR development. France implemented a pilot EPR scheme for single-use medical devices in 2024, requiring manufacturers selling more than 10,000 units annually to register with a producer responsibility organization and contribute to waste management funding. Germany followed with similar regulations in 2025, focusing specifically on examination gloves and surgical gloves as priority waste streams.
Key components of medical glove EPR programs include:
- Mandatory registration and reporting of glove sales volumes by manufacturers
- Financial contributions calculated per unit sold or by weight
- Minimum recycled content requirements (typically 10-30% by 2028 in EU proposals)
- Take-back infrastructure requirements for large healthcare facilities
- Public reporting of collection and recycling rates
- Penalties for non-compliance ranging from fines to market access restrictions
In the United States, EPR for medical gloves remains voluntary as of 2026. California and Washington have explored legislation but face opposition from healthcare industry groups concerned about cost increases and contamination liability. However, several major hospital systems including Kaiser Permanente and Cleveland Clinic have negotiated voluntary EPR-style agreements with suppliers.
Choose EPR-based purchasing if: Your facility is in an EU member state with mandatory compliance, you have leverage to negotiate take-back terms with suppliers, or you want to shift waste management costs off your operating budget. EPR works best for large healthcare systems with centralized purchasing power.
A common mistake is assuming EPR eliminates all hospital responsibilities. Even under EPR frameworks, healthcare facilities must still segregate gloves properly, maintain contamination controls, and coordinate with collection programs. The responsibility shifts, but operational requirements remain.
How Do Hospital Nitrile Glove Recycling Programs Actually Work
Hospital nitrile glove recycling programs operate through specialized collection systems that segregate non-contaminated gloves from general waste, followed by shipment to processing facilities that convert the material into new products. The process requires strict protocols to prevent contamination, dedicated collection infrastructure, and partnerships with certified recyclers.
The typical workflow includes these steps:
Segregation at point of use: Staff place used gloves in designated blue or green bins located in non-clinical areas like administrative offices, food service, maintenance departments, and non-infectious patient care zones.
Contamination screening: Only gloves from approved low-risk areas enter the recycling stream. Gloves from surgical suites, emergency departments, isolation rooms, or any infectious disease treatment areas go to medical waste incineration.
Collection and storage: Facilities consolidate gloves in larger containers, typically 40-60 gallon bins or gaylord boxes, stored in designated areas until pickup.
Transportation: Recycling partners collect filled containers on scheduled routes, usually every 2-4 weeks depending on volume.
Processing: At recycling facilities, gloves undergo shredding, cleaning, and conversion into crumb rubber or pelletized material for manufacturing new products.
The largest hospital recycling program in North America is operated by RightCycle, a Kimberly-Clark initiative launched in 2011. As of 2026, the program operates in over 800 healthcare facilities across the US and Canada, processing approximately 2.3 million pounds of nitrile gloves annually. Participating hospitals report diverting 35-55% of their total glove waste from landfills.
Critical success factors include:
- Clear visual signage: Color-coded bins with pictures showing acceptable items reduce contamination rates from 15-20% to under 5%
- Staff training: Initial training plus quarterly refreshers maintain compliance; facilities with annual-only training see 3x higher contamination
- Leadership buy-in: Programs with executive sponsorship achieve 60% higher participation rates than grassroots initiatives
- Convenient placement: Bins must be within 10 feet of glove use areas or participation drops by 40%
A common mistake is placing recycling bins in clinical areas where contamination risk is high. This creates safety hazards and can disqualify entire batches of collected material. Instead, focus collection efforts on administrative buildings, outpatient clinics, and food service areas where contamination risk is minimal.
For hospitals interested in learning more about nitrile gloves used in healthcare settings, understanding the different types and their applications helps identify which gloves are suitable for recycling programs.
Can Nitrile Gloves Be Recycled or Are They Just Trash
Nitrile gloves can be recycled through specialized processes, but they cannot go into standard municipal recycling bins and require dedicated collection programs. The synthetic rubber material (acrylonitrile butadiene rubber) is technically recyclable, but contamination concerns and the lack of widespread infrastructure mean most nitrile gloves still end up in landfills or incinerators.
The recycling process differs fundamentally from paper or plastic recycling. Nitrile gloves are shredded into small pieces, cleaned to remove residues, then processed through one of two methods: mechanical recycling that converts them into crumb rubber, or chemical recycling that breaks down the polymer chains for reprocessing. The resulting material typically becomes lower-grade products rather than new gloves due to quality requirements for medical devices.
Products commonly made from recycled nitrile gloves:
- Playground surfaces and safety padding
- Outdoor athletic tracks and sports flooring
- Industrial floor mats and anti-fatigue mats
- Automotive parts like mud flaps and floor liners
- Construction materials including rubberized asphalt
- Landscaping mulch and weed barriers
The technical recyclability of nitrile gloves has been proven, but economic viability remains challenging. Processing costs range from $0.40 to $0.80 per pound, while virgin nitrile rubber costs $1.20 to $1.80 per pound. This narrow margin means recycling programs depend on volume, efficient logistics, and sometimes subsidies or EPR funding to remain financially sustainable.
Contamination is the primary barrier to widespread nitrile glove recycling. Gloves exposed to chemotherapy drugs, infectious agents, or hazardous chemicals cannot enter recycling streams due to safety regulations and the risk of contaminating finished products. This eliminates approximately 60-70% of hospital glove waste from recycling eligibility.
Choose recycling if: Your gloves come from administrative areas, food service, non-infectious patient care, maintenance work, or other low-contamination environments. Avoid recycling gloves from surgical suites, emergency departments, oncology units, or any area treating infectious diseases.
For more details on the recycling process and technical considerations, see our guide on whether nitrile gloves can be recycled.
EPR vs Traditional Waste Management for Disposable Gloves
EPR and traditional waste management for disposable gloves differ fundamentally in who pays, who manages logistics, and what incentives drive product design. Traditional systems place all costs and responsibilities on healthcare facilities and municipalities, while EPR shifts these burdens to manufacturers who profit from glove sales.
Traditional waste management model:
- Hospitals pay for all waste collection, transportation, and disposal
- Costs typically range from $0.08-0.12 per pound for landfill, $0.15-0.25 per pound for incineration
- No financial incentive for manufacturers to reduce material use or improve recyclability
- Waste management is a pure cost center with no revenue offset
- Municipalities bear long-term environmental costs of landfills
EPR model:
- Manufacturers pay fees based on units sold or weight of products
- Fees fund collection infrastructure, recycling facilities, and program administration
- Creates direct financial incentive for manufacturers to design recyclable products and reduce material use
- Hospitals may pay reduced or zero disposal fees for gloves in EPR programs
- Environmental costs are internalized into product pricing
A 500-bed hospital using approximately 8 million gloves annually spends roughly $35,000-$45,000 on glove waste disposal under traditional systems. Under EPR frameworks with manufacturer-funded take-back programs, direct disposal costs can drop to $15,000-$25,000, though glove purchase prices may increase by 2-8% as manufacturers pass through EPR compliance costs.
The net financial impact varies by facility size and local waste disposal costs. Large academic medical centers with high waste disposal fees typically see net savings of 15-25% on total glove lifecycle costs under EPR. Smaller facilities in areas with low landfill costs may see minimal savings or slight cost increases.
Beyond direct costs, EPR offers these advantages:
- Reduced administrative burden as manufacturers handle logistics
- Improved sustainability metrics for hospital reporting
- Potential regulatory compliance benefits in jurisdictions with mandatory EPR
- Marketing value for environmentally conscious patients and staff
Traditional systems remain preferable when: EPR programs are unavailable in your region, your facility has very low waste disposal costs, or you lack the staff capacity to implement segregation and collection protocols required by EPR programs.
A common mistake is assuming EPR is always cheaper. In rural areas with low landfill costs and limited recycling infrastructure, traditional disposal may cost less. Calculate total lifecycle costs including staff time, storage space, and potential purchase price increases before committing to EPR programs.
How Much Does It Cost Hospitals to Recycle Nitrile Gloves
Recycling nitrile gloves costs hospitals approximately $0.15-0.30 per pound for collection and processing, compared to $0.08-0.12 per pound for landfill disposal. However, total waste management costs often decrease because recycling programs typically include free or subsidized collection containers, reduced pickup frequency for general waste, and potential rebates from EPR programs.
Detailed cost breakdown for a 300-bed hospital:
| Cost Component | Annual Amount | Notes |
|---|---|---|
| Collection bins and signage | $800-1,500 | One-time setup, 15-25 bins |
| Staff training | $1,200-2,000 | Initial plus quarterly refreshers |
| Storage space | $0-500 | Often uses existing space |
| Recycling pickup and processing | $4,500-7,500 | Based on 25,000-30,000 lbs/year |
| Program administration | $1,000-2,000 | Coordinator time, reporting |
| Total recycling costs | $7,500-13,500 | |
| Traditional disposal (same volume) | $2,000-3,600 | Landfill only |
| Reduced general waste disposal | -$3,000-5,000 | Fewer pickups needed |
| Net additional cost | $2,500-7,900 |
The cost per pound decreases significantly with volume. Facilities processing over 50,000 pounds annually often negotiate rates of $0.10-0.15 per pound, making recycling cost-competitive with landfill disposal even before accounting for indirect savings.
Hidden costs to consider:
- Staff time for sorting and monitoring (typically 2-4 hours per week)
- Contamination incidents that disqualify batches (can add 10-15% to costs)
- Storage space for accumulating materials between pickups
- Potential increases in glove purchase prices if manufacturers pass through EPR costs
Cost-saving strategies:
- Join regional consortiums to achieve volume discounts (reduces per-pound costs by 20-40%)
- Negotiate with glove suppliers to include recycling in purchasing contracts
- Focus collection on high-volume, low-contamination areas first
- Use existing waste management staff rather than hiring dedicated personnel
- Apply for sustainability grants that many states and healthcare associations offer
A 150-bed community hospital in Ohio reported total first-year recycling costs of $8,200 while diverting 18,000 pounds of gloves from landfills. Their traditional disposal cost for the same volume would have been $2,160, creating a net additional cost of $6,040. However, they received a $3,500 state sustainability grant and reduced general waste pickups by one per week, saving $2,800 annually, bringing net additional cost to approximately $260 per year.
Choose recycling despite higher costs if: Sustainability is a strategic priority, you’re pursuing green building certifications, your community has high landfill costs or limited capacity, or you face regulatory pressure to reduce waste.

Which Glove Manufacturers Have Take-Back Programs
Kimberly-Clark, Halyard Health, Cardinal Health, and Medline Industries currently operate the largest take-back programs for nitrile gloves in North America as of 2026. These programs vary significantly in geographic availability, eligibility requirements, and whether they charge fees or offer free collection.
Kimberly-Clark RightCycle Program:
- Available in US, Canada, and select European markets
- Accepts nitrile gloves, face masks, and other PPE
- Free collection for facilities generating 200+ pounds per quarter
- Smaller generators can participate through regional consolidation partners
- Processes approximately 2.3 million pounds of gloves annually
- No requirement to purchase Kimberly-Clark products exclusively
Halyard Health WRAP Program (Waste Reduction and Packaging):
- Operates in US healthcare facilities
- Requires minimum 300 pounds per pickup
- Charges $0.18-0.25 per pound depending on volume and location
- Accepts only Halyard-branded gloves and select competitor products
- Provides detailed sustainability reporting for hospital environmental programs
Cardinal Health Sustainable Solutions:
- Available to Cardinal Health distribution customers
- Free collection for facilities with annual glove purchases exceeding $50,000
- Accepts multiple brands of nitrile gloves
- Integrated with existing Cardinal delivery routes to reduce transportation costs
- Launched in 2023, now serves approximately 400 facilities
Medline ReNewal Program:
- Operates in 35 US states as of 2026
- Charges $0.20-0.30 per pound for collection and processing
- Accepts Medline and competitor gloves
- Offers carbon offset credits for participating facilities
- Minimum 150 pounds per quarterly pickup
International programs:
- Ansell Earth (Australia, New Zealand, UK): Free collection for facilities using 10,000+ gloves monthly
- Sempermed Green Program (Austria, Germany, Switzerland): Mandatory participation under EU EPR regulations, funded through product pricing
- Hartalega Sustainability Initiative (Malaysia, Singapore): Pilot program accepting gloves for conversion to construction materials
Most programs require facilities to segregate gloves by contamination risk and provide documentation that collected materials come from approved low-risk areas. Programs typically exclude gloves from surgical suites, emergency departments, and infectious disease units.
Common eligibility requirements across programs:
- Minimum volume thresholds (typically 150-300 pounds per pickup)
- Contamination protocols and staff training documentation
- Dedicated collection infrastructure (bins, storage area)
- Signed participation agreements with liability waivers
- Quarterly or annual reporting of volumes collected
A common mistake is assuming take-back programs are universally available. Geographic coverage remains limited, with rural areas and smaller markets often excluded due to transportation costs. Before committing to a specific glove brand, verify that take-back services actually operate in your location.
For facilities exploring alternatives to disposable nitrile gloves that might reduce overall waste, reusable options exist for certain non-clinical applications, though they introduce different cost and hygiene considerations.
What Are the Biggest Mistakes Hospitals Make with Glove Waste Reduction
The most critical mistake hospitals make with glove waste reduction is mixing contaminated and non-contaminated gloves in recycling bins, which disqualifies entire batches and creates safety hazards. This single error accounts for approximately 40% of program failures and can expose facilities to regulatory violations and liability.
Top implementation mistakes and how to avoid them:
1. Inadequate contamination protocols
Placing recycling bins in clinical areas where infectious disease treatment occurs leads to contaminated gloves entering the recycling stream. This violates safety regulations and can shut down entire programs.
Solution: Limit collection to administrative areas, food service, maintenance, and non-infectious patient care only. Use clear signage stating “No gloves from patient care areas” and conduct monthly audits.
2. Insufficient staff training
One-time training sessions result in 60-70% knowledge retention after six months. Staff forget protocols, new employees miss training, and contamination rates increase.
Solution: Implement quarterly refresher training, include glove recycling in new employee orientation, and use visual reminders at collection points. Facilities with ongoing training maintain contamination rates under 5%.
3. Underestimating logistics and storage needs
Hospitals often fail to allocate adequate space for accumulating gloves between pickups. A 300-bed facility generates 500-700 pounds of recyclable gloves monthly, requiring approximately 60-80 cubic feet of storage space.
Solution: Designate a specific storage area with climate control (nitrile degrades in extreme heat), easy loading dock access, and clear labeling. Calculate storage needs at 2-3 cubic feet per 10 pounds of monthly volume.
4. Focusing only on clinical areas
Many programs concentrate collection efforts in patient care areas where contamination risk is highest and participation rates are lowest due to infection control concerns.
Solution: Start with administrative buildings, outpatient clinics, and food service where contamination risk is minimal and participation rates exceed 70%. Expand to low-risk clinical areas only after establishing successful operations.
5. Ignoring cost-benefit analysis
Hospitals implement recycling programs without calculating total lifecycle costs, then face budget pressure when costs exceed expectations.
Solution: Calculate costs including staff time, storage, collection fees, and potential glove price increases. Compare against current disposal costs plus any sustainability grants or EPR rebates. Set realistic budget expectations before launch.
6. Poor communication with environmental services
Recycling programs often operate independently from existing waste management systems, creating confusion and operational conflicts.
Solution: Integrate glove recycling into existing environmental services workflows. Train waste management staff first, as they’ll be program champions or obstacles depending on their buy-in.
7. Unrealistic volume expectations
Hospitals overestimate recyclable glove volumes by 50-100% because they fail to account for contamination exclusions and participation rates.
Solution: Estimate that only 30-40% of total glove waste qualifies for recycling in typical hospitals. Use this conservative estimate for vendor negotiations and budget planning.
8. Neglecting program metrics and reporting
Without tracking volumes, contamination rates, costs, and participation, programs drift and lose momentum.
Solution: Establish monthly reporting including pounds collected, contamination incidents, cost per pound, and participation rates by department. Share results with leadership and staff to maintain engagement.
A 400-bed hospital in Michigan launched a glove recycling program in 2024 that failed within eight months due to multiple mistakes: they placed bins in emergency departments and surgical suites (contamination), provided only initial training (knowledge decay), and didn’t allocate storage space (logistics failure). After relaunch with corrected protocols focused on administrative areas, quarterly training, and dedicated storage, the program successfully diverted 22,000 pounds in its first year.
Are Nitrile Glove Recycling Programs Worth It for Small Clinics
Nitrile glove recycling programs are financially challenging for small clinics with fewer than 50 employees due to high per-unit costs, minimum volume requirements, and limited staff capacity for program management. However, clinics can achieve viability by joining regional consortiums, partnering with larger healthcare systems, or focusing on sustainability value beyond direct cost savings.
A typical small clinic (10-20 employees) uses approximately 50,000-100,000 gloves annually, generating 300-600 pounds of potentially recyclable glove waste. At standard recycling rates of $0.20-0.30 per pound, annual recycling costs would be $60-180 compared to $24-72 for landfill disposal, creating a net additional cost of $36-108.
However, this simple calculation misses several factors:
Barriers for small clinics:
- Most take-back programs require 150-300 pound minimum pickups, meaning small clinics must store gloves for 6-12 months
- Storage space is limited and valuable in small facilities
- Staff time for program management represents a higher percentage of total labor in small operations
- Transportation costs per pound are 3-5x higher for small-volume pickups
- Limited negotiating power with recycling vendors
Strategies that make programs viable:
1. Regional consortiums: Groups of 5-15 small clinics pool volumes and share a central collection point. This achieves the 300-500 pound quarterly volumes needed for cost-effective pickup while distributing program management across multiple facilities.
2. Piggyback on larger systems: Small clinics affiliated with hospital systems can often add their gloves to the hospital’s recycling program at minimal incremental cost.
3. Focus on high-value areas: Collect only from administrative offices and break rooms where contamination risk is zero and collection is simple. This reduces program complexity while still demonstrating environmental commitment.
4. Sustainability grants: Many state healthcare associations and environmental agencies offer $500-2,000 grants for small clinics implementing waste reduction programs. These grants can fund 2-5 years of recycling costs.
5. Marketing value: For clinics competing on environmental credentials, the cost of recycling may be justified by patient attraction and retention even if direct financial ROI is negative.
A dental clinic in Oregon with 12 employees joined a regional consortium of eight practices in 2025. Individually, each clinic generated only 40-60 pounds of recyclable gloves quarterly. Together, they accumulated 350-450 pounds, qualifying for quarterly pickups at $0.18 per pound. Each clinic pays approximately $30 quarterly ($120 annually) compared to $18 for traditional disposal, but they received a $1,200 state grant that funded the program for all eight clinics for two years.
Choose recycling if: You can join a consortium, your clinic has strong sustainability values that attract patients, you’re pursuing green certifications, or you have access to grants. Skip recycling if you’re operating independently with tight margins and no sustainability differentiation in your market.
Alternative approaches for small clinics:
- Reduce glove usage through appropriate use protocols (can cut consumption 15-25%)
- Switch to thinner gloves that meet clinical needs but use less material
- Negotiate with suppliers for take-back programs as part of purchasing contracts
- Focus on other waste streams with better economics (paper, cardboard, metals)
What Happens to Nitrile Gloves After They Get Recycled
Recycled nitrile gloves are processed into crumb rubber or pelletized material that becomes playground surfaces, athletic tracks, industrial mats, automotive parts, and construction materials. The gloves cannot be recycled back into new medical-grade gloves due to contamination concerns and the quality requirements for medical devices.
The recycling process involves these steps:
1. Collection and sorting (at hospital): Gloves are segregated from other waste and stored in dedicated containers.
2. Transportation: Collected gloves are shipped to specialized recycling facilities, typically in truckload quantities of 20,000-40,000 pounds.
3. Initial processing: Gloves are shredded into small pieces (typically 0.5-2 inch fragments) using industrial shredders.
4. Cleaning: Shredded material undergoes washing to remove residues, oils, and contaminants. This step is critical for product quality and safety.
5. Size reduction: Clean fragments are ground into finer crumb rubber (typically 10-40 mesh size, roughly 0.4-2mm particles).
6. Quality testing: Samples are tested for contamination, particle size distribution, and material properties.
7. Manufacturing: Crumb rubber is mixed with binders and other materials to create finished products.
Common products made from recycled nitrile gloves:
- Playground surfaces: Poured-in-place rubber surfacing and rubber tiles for playgrounds and play areas
- Athletic surfaces: Running tracks, gym flooring, and sports court surfaces
- Industrial products: Anti-fatigue mats for factories and warehouses, industrial floor tiles
- Automotive parts: Mud flaps, floor mats, and sound dampening materials
- Construction materials: Rubberized asphalt, roofing materials, and waterproofing membranes
- Landscaping products: Rubber mulch, weed barriers, and erosion control materials
The material properties of recycled nitrile make it particularly suitable for applications requiring durability, weather resistance, and cushioning. Nitrile rubber maintains flexibility across wide temperature ranges and resists degradation from oils, chemicals, and UV exposure better than natural rubber.
Quality considerations:
Recycled nitrile from medical gloves is typically classified as “post-consumer recycled content” and commands lower prices than virgin nitrile rubber. A pound of virgin nitrile costs $1.20-1.80, while recycled nitrile crumb sells for $0.30-0.60 per pound. This price difference reflects the processing costs, quality variability, and contamination concerns.
The recycling process is not infinitely repeatable. Each recycling cycle degrades the polymer chains slightly, reducing material properties. Most recycled nitrile products contain 30-70% recycled content mixed with virgin rubber and other materials to achieve required performance specifications.
Environmental impact:
Recycling nitrile gloves reduces landfill waste and conserves petroleum resources used in virgin nitrile production. However, the environmental benefit is modest compared to recycling materials like aluminum or paper because nitrile recycling is energy-intensive and produces lower-value products. Life cycle assessments suggest recycling nitrile gloves reduces environmental impact by 20-35% compared to landfill disposal, primarily through avoided methane emissions and reduced virgin material extraction.
A common misconception is that recycled gloves become new gloves, creating a closed-loop system. This is technically possible but economically and regulatorily impractical for medical devices. The FDA and similar agencies require medical gloves to meet strict quality standards that are difficult to achieve with recycled content.
Do Contaminated Medical Gloves Qualify for Recycling Programs
Contaminated medical gloves from surgical procedures, infectious disease treatment, chemotherapy administration, or exposure to hazardous chemicals do not qualify for standard recycling programs and must be disposed of through medical waste incineration. The contamination creates safety hazards for recycling workers and can compromise the safety of finished products made from recycled material.
Gloves that are excluded from recycling:
- Surgical gloves from operating rooms and procedure suites
- Gloves from emergency departments and trauma care
- Gloves used in isolation rooms or infectious disease treatment
- Gloves exposed to chemotherapy drugs or hazardous pharmaceuticals
- Gloves contaminated with blood, body fluids, or tissue
- Gloves used in pathology and laboratory work with infectious agents
- Gloves from dental procedures involving blood exposure
- Gloves used with radioactive materials
These exclusions typically represent 60-70% of total glove usage in acute care hospitals, leaving only 30-40% potentially eligible for recycling.
Gloves that may qualify for recycling:
- Gloves from administrative offices and non-clinical areas
- Gloves used in food service and dietary departments
- Gloves from maintenance and housekeeping (if not exposed to hazardous chemicals)
- Gloves from outpatient clinics for routine, non-infectious care
- Gloves used in physical therapy and rehabilitation
- Gloves from pharmacy (excluding chemotherapy preparation)
The distinction between contaminated and non-contaminated gloves is not always clear-cut, creating gray areas that require facility-specific risk assessment and policy development.
Risk assessment framework:
Low risk (generally acceptable for recycling):
- No contact with blood, body fluids, or infectious agents
- Used in areas where patients are not being treated for infectious diseases
- No exposure to chemotherapy drugs or hazardous chemicals
- Administrative or support functions only
Medium risk (requires evaluation):
- Contact with intact skin only
- Used in outpatient settings with low infection prevalence
- Exposure to cleaning chemicals or non-hazardous substances
- Requires facility-specific protocols and risk assessment
High risk (exclude from recycling):
- Any contact with blood, body fluids, mucous membranes, or non-intact skin
- Used in areas treating infectious diseases
- Exposure to chemotherapy drugs, radioactive materials, or hazardous chemicals
- Surgical or invasive procedures
Regulatory considerations:
The EPA does not specifically regulate nitrile glove recycling, but general medical waste regulations apply. Gloves contaminated with infectious agents are classified as regulated medical waste and must be treated (typically through incineration or autoclaving) before disposal. State regulations vary, with some states having more restrictive definitions of medical waste than federal standards.
OSHA regulations protect workers handling potentially contaminated materials. Recycling programs must ensure that collected gloves do not expose workers to bloodborne pathogens or hazardous chemicals. This requires clear segregation protocols and documentation that gloves come from approved low-risk areas.
A common mistake is attempting to recycle gloves from “clean” patient care areas like medical-surgical units. Even routine patient care involves contamination risks that disqualify gloves from recycling. Unless the area is specifically designated as non-infectious and gloves have no patient contact, they should be excluded.
Verification and auditing:
Successful programs implement regular audits to verify contamination protocols are being followed. This typically includes:
- Monthly visual inspection of collection bins for obviously contaminated gloves
- Quarterly random sampling and testing for biological contamination
- Annual review of collection areas to ensure they remain low-risk
- Incident reporting system for contamination events
One contamination incident can disqualify an entire batch of collected gloves (typically 500-1,000 pounds), creating significant cost and safety issues. Facilities with contamination rates above 5% often find recycling programs become economically unviable.
Alternatives to Nitrile Gloves That Produce Less Waste
Reusable gloves, biodegradable glove materials, and right-sizing protocols that reduce unnecessary glove usage represent the primary alternatives to disposable nitrile gloves for waste reduction. Each alternative involves trade-offs between waste reduction, cost, infection control, and operational complexity.
Reusable gloves:
Heavy-duty reusable gloves made from neoprene, latex, or thick nitrile can be cleaned and reused 50-200 times before disposal. These work well for housekeeping, food service, maintenance, and some laboratory applications but are inappropriate for patient care due to infection control concerns.
Advantages:
- Reduce waste by 95-98% compared to disposable gloves
- Lower long-term costs after initial investment
- Better durability for heavy-duty tasks
- Reduced supply chain vulnerability
Disadvantages:
- Higher upfront cost ($3-15 per pair vs. $0.05-0.15 for disposable)
- Require cleaning infrastructure and protocols
- Not suitable for patient care or sterile procedures
- Risk of cross-contamination if cleaning is inadequate
- Staff resistance due to comfort and convenience preferences
A 200-bed hospital in Vermont replaced disposable gloves with reusable gloves in housekeeping and food service departments in 2024, eliminating approximately 180,000 disposable gloves annually (1,200 pounds of waste). Initial investment was $4,500 for 300 pairs of reusable gloves plus $2,000 for cleaning equipment. Annual savings exceeded $8,000 after accounting for cleaning costs.
Biodegradable and compostable gloves:
Several manufacturers now offer gloves made from biodegradable materials including modified nitrile, polyhydroxyalkanoates (PHA), and plant-based polymers. These gloves break down in industrial composting facilities or landfills faster than conventional nitrile.
Advantages:
- Reduce long-term environmental impact
- Similar performance to conventional nitrile for many applications
- Can be disposed of with organic waste in some facilities
Disadvantages:
- Cost 30-80% more than conventional nitrile gloves
- Require industrial composting facilities (not available in many areas)
- Degradation time still measured in years, not weeks or months
- Performance may be inferior for chemical resistance
- Limited availability and supplier options
As of 2026, biodegradable gloves represent less than 2% of the medical glove market due to cost and performance limitations. They work best for food service and light-duty applications rather than clinical use.
Right-sizing and appropriate use protocols:
Many healthcare facilities overuse gloves, with staff wearing them for tasks that don’t require hand protection. Implementing appropriate use protocols can reduce glove consumption by 15-30% without compromising safety.
Strategies include:
- Training on when gloves are actually required vs. when hand hygiene alone is sufficient
- Removing glove boxes from areas where they’re not needed
- Switching to thinner gloves (3-4 mil instead of 5-6 mil) for applications where thinner gloves provide adequate protection
- Implementing “glove audits” to identify overuse patterns
- Using visual reminders about appropriate glove use
A study at Johns Hopkins Hospital found that 23% of glove use in non-clinical areas was unnecessary and could be eliminated through staff education and protocol changes. This reduced annual glove consumption by 1.8 million gloves without any adverse safety outcomes.
Hybrid approaches:
The most effective waste reduction strategies combine multiple approaches:
- Reusable gloves for housekeeping and food service
- Thinner disposable gloves for routine patient care
- Standard nitrile gloves for high-risk procedures
- Recycling programs for non-contaminated disposable gloves
- Appropriate use protocols to eliminate unnecessary glove use
For facilities interested in exploring alternatives to disposable nitrile gloves, a comprehensive evaluation of use cases, costs, and infection control requirements is essential before making changes.
How to Start a Glove Recycling Program in My Hospital
Starting a hospital glove recycling program requires six key steps: conducting a waste audit to quantify recyclable volumes, identifying a recycling partner, developing contamination protocols, implementing collection infrastructure, training staff, and establishing metrics for ongoing management. Most programs take 3-6 months from planning to full implementation.
Step 1: Conduct a waste audit (2-4 weeks)
Measure current glove usage and waste generation to establish baseline data and identify high-volume, low-contamination areas.
Actions:
- Survey all departments to estimate monthly glove usage
- Identify areas where gloves are used but contamination risk is low (administrative, food service, outpatient clinics)
- Calculate total potentially recyclable volume (typically 30-40% of total glove waste)
- Document current waste disposal costs for comparison
A 300-bed hospital typically generates 25,000-35,000 pounds of potentially recyclable glove waste annually. Use this as a benchmark for initial estimates.
Step 2: Identify recycling partners (2-3 weeks)
Research available programs and negotiate terms based on your volume and location.
Actions:
- Contact major manufacturers (Kimberly-Clark, Halyard, Cardinal Health, Medline) about take-back programs
- Research regional recycling companies that accept nitrile gloves
- Request quotes including collection frequency, minimum volumes, and per-pound costs
- Verify that programs accept multiple glove brands or negotiate with your current supplier
- Check references from other hospitals using the program
Step 3: Develop contamination protocols (1-2 weeks)
Create clear policies defining which gloves can be recycled and which must go to medical waste.
Actions:
- Designate approved collection areas (administrative buildings, food service, maintenance, select outpatient areas)
- Explicitly exclude high-risk areas (surgical suites, emergency departments, isolation rooms, oncology)
- Create visual decision aids for staff (“Can this glove be recycled?” flowcharts)
- Develop incident response procedures for contamination events
- Obtain legal and infection control department approval
Step 4: Implement collection infrastructure (2-4 weeks)
Install bins, signage, and storage systems to support the program.
Actions:
- Purchase or obtain collection bins (typically 15-25 bins for a 300-bed hospital)
- Create clear, visual signage with pictures showing acceptable items
- Designate central storage area for accumulated gloves (60-100 cubic feet for quarterly pickups)
- Establish pickup schedule with recycling partner
- Integrate with existing waste management workflows
Budget for infrastructure:
- Collection bins: $30-60 each (15-25 bins = $450-1,500)
- Signage and labels: $200-400
- Storage containers: $100-300
- Total initial investment: $750-2,200
Step 5: Train staff (ongoing)
Comprehensive training is the single most important factor in program success.
Actions:
- Conduct initial training for all staff in participating departments (30-45 minute sessions)
- Create quick reference guides and post at collection points
- Train environmental services staff as program champions
- Include glove recycling in new employee orientation
- Schedule quarterly refresher training
- Establish feedback mechanisms for staff questions and concerns
Step 6: Establish metrics and reporting (ongoing)
Track program performance to demonstrate value and identify improvement opportunities.
Key metrics to monitor:
- Pounds of gloves recycled monthly/quarterly
- Contamination rate (target: under 5%)
- Cost per pound recycled
- Participation rate by department
- Total waste reduction percentage
- Cost savings or additional costs vs. baseline
Implementation timeline:
- Month 1: Waste audit, partner research, leadership approval
- Month 2: Partner selection, protocol development, infrastructure ordering
- Month 3: Infrastructure installation, staff training begins
- Month 4: Pilot launch in 2-3 departments
- Month 5: Evaluation and adjustment of pilot
- Month 6: Full rollout to all approved areas
Common pitfalls to avoid:
- Starting too big: Launch in 2-3 departments first, then expand after proving the model
- Inadequate training: Budget for ongoing training, not just initial sessions
- Poor communication: Keep staff informed about program goals, progress, and their role
- Ignoring feedback: Create channels for staff to report problems and suggest improvements
- Unrealistic expectations: Set conservative volume and cost targets initially
A 250-bed community hospital in Wisconsin followed this process in 2025, launching their program in administrative buildings and outpatient clinics first. After three months, they expanded to medical-surgical units for gloves used in non-patient-contact activities. First-year results: 19,000 pounds recycled, 4% contamination rate, net additional cost of $3,200 after accounting for reduced general waste disposal.
Why Aren’t More Hospitals Recycling Nitrile Gloves If It’s Possible
Most hospitals don’t recycle nitrile gloves because of contamination concerns, limited recycling infrastructure availability, higher costs compared to landfill disposal, staff capacity constraints, and lack of regulatory requirements or financial incentives. Despite technical feasibility, these practical barriers prevent widespread adoption.
Primary barriers to adoption:
1. Contamination liability and safety concerns (cited by 68% of hospitals in a 2025 survey)
Healthcare administrators worry that recycling programs create infection control risks and potential liability if contaminated gloves enter recycling streams. Even though protocols can minimize these risks, the perceived liability often outweighs sustainability benefits.
2. Higher direct costs (cited by 61%)
Recycling costs $0.15-0.30 per pound compared to $0.08-0.12 for landfill disposal in most markets. Without EPR funding or sustainability mandates, the business case is weak, especially for hospitals with tight margins.
3. Limited geographic availability (cited by 54%)
Take-back programs operate primarily in major metropolitan areas and regions with existing recycling infrastructure. Rural hospitals and facilities in smaller markets often have no access to recycling services regardless of their interest.
4. Staff capacity and competing priorities (cited by 49%)
Implementing recycling programs requires staff time for training, monitoring, and program management. With healthcare workforce shortages and competing clinical priorities, sustainability initiatives often get deprioritized.
5. Lack of regulatory requirements (cited by 43%)
Unlike the EU where EPR regulations are creating mandatory participation, US hospitals face no legal requirement to recycle gloves. Without regulatory pressure, voluntary adoption remains low.
6. Complexity of segregation protocols (cited by 38%)
Distinguishing between recyclable and non-recyclable gloves requires judgment calls that frontline staff find confusing. The risk of mistakes leads many facilities to avoid recycling entirely rather than risk contamination incidents.
7. Inadequate storage space (cited by 31%)
Accumulating gloves for quarterly pickups requires 60-100 cubic feet of storage space that many facilities don’t have available, especially in urban hospitals with limited square footage.
Adoption patterns:
As of 2026, approximately 12-15% of US hospitals have active nitrile glove recycling programs, concentrated in:
- Large academic medical centers with dedicated sustainability staff
- Healthcare systems with corporate sustainability commitments
- Facilities in states with strong environmental regulations (California, Washington, Oregon, Massachusetts)
- Hospitals pursuing green building certifications (LEED, Green Guide for Health Care)
Adoption is significantly higher in the EU (estimated 35-40%) due to EPR regulations and stronger cultural emphasis on waste reduction.
What would drive increased adoption:
Regulatory mandates: EPR regulations requiring manufacturer take-back programs would eliminate the cost barrier and create universal access to recycling infrastructure.
Financial incentives: Grants, tax credits, or disposal fee structures that make recycling cost-competitive with landfill disposal would improve business cases.
Simplified protocols: Standardized, industry-wide contamination protocols would reduce complexity and liability concerns.
Integrated solutions: Recycling programs built into glove purchasing contracts would eliminate the need for separate vendor relationships and program management.
Peer pressure: As more prestigious healthcare systems adopt recycling, competitive pressure may drive broader adoption even without regulatory requirements.
A healthcare sustainability director at a 400-bed hospital explained their decision not to implement glove recycling: “We ran the numbers and it would cost us an additional $12,000 annually with significant staff time investment. We don’t have regulatory pressure, our community doesn’t prioritize this issue, and we have other sustainability initiatives with better ROI. Until the economics change or we face requirements, it’s not a priority.”
This pragmatic cost-benefit analysis reflects the reality for many hospitals. Glove recycling remains a niche practice for facilities with strong sustainability commitments rather than a mainstream waste management strategy.
What Regulations Exist for Medical Glove Waste and EPR
As of 2026, the European Union has implemented Extended Producer Responsibility regulations for medical gloves in France and Germany, with EU-wide standards under development, while the United States has no federal EPR requirements and only voluntary state-level initiatives. Existing regulations focus primarily on medical waste disposal rather than recycling or producer responsibility.
European Union:
France: Implemented EPR for single-use medical devices including gloves in January 2024 under the Anti-Waste for a Circular Economy (AGEC) law. Requirements include:
- Manufacturers selling more than 10,000 units annually must register with an approved producer responsibility organization
- Financial contributions of approximately 0.002-0.005 euros per glove unit
- Minimum 15% recycled content requirement by 2028
- Annual reporting of sales volumes and recycling rates
- Penalties up to 30,000 euros for non-compliance
Germany: Launched EPR pilot program for examination and surgical gloves in March 2025 under the Circular Economy Act. Key provisions:
- Mandatory participation for manufacturers with annual sales exceeding 50,000 euros
- Contribution rates of 0.003-0.006 euros per unit based on recyclability
- Take-back infrastructure requirements for hospitals using more than 500,000 gloves annually
- Target of 25% collection rate by 2027, 40% by 2030
- Fines up to 100,000 euros for non-compliance
EU-wide standards: The European Commission is developing harmonized EPR standards for medical gloves expected to take effect in 2027-2028. Proposed requirements include:
- Mandatory EPR across all member states
- Standardized contribution rates and reporting formats
- Minimum 20% recycled content by 2030
- Eco-design requirements favoring recyclable materials
- Common contamination protocols and safety standards
United States:
Federal level: No EPR regulations exist for medical gloves. The EPA has identified medical gloves as a priority waste stream for potential future regulation but has not proposed specific requirements as of 2026.
State level:
California: Proposed but not enacted legislation (AB 2026) would require manufacturers to establish take-back programs for single-use medical devices including gloves. The bill stalled in committee in 2025 due to healthcare industry opposition.
Washington: Exploring EPR framework as part of broader medical waste reduction initiative. Public comment period concluded in late 2025 with regulations potentially taking effect in 2027.
Oregon: Voluntary EPR pilot program launched in 2024 with state funding. Manufacturers receive tax credits for establishing take-back programs, but participation is optional.
Existing medical waste regulations:
While EPR regulations are limited, all jurisdictions have medical waste disposal regulations that affect glove waste management:
Federal (US):
- EPA regulates medical waste under the Resource Conservation and Recovery Act (RCRA)
- OSHA Bloodborne Pathogens Standard requires proper handling of contaminated gloves
- Gloves contaminated with infectious agents must be treated before disposal
State regulations vary significantly:
- Some states classify all gloves from patient care areas as regulated medical waste requiring incineration
- Others allow gloves without visible contamination to be disposed as general waste
- A few states offer reduced disposal fees for facilities with active recycling programs
International:
Canada: No federal EPR for gloves, but British Columbia and Ontario have voluntary programs with provincial funding support.
Australia: National Waste Policy includes medical gloves as priority waste stream. EPR framework under development with implementation expected 2027-2028.
United Kingdom: Post-Brexit, developing independent EPR standards separate from EU. Consultation phase ongoing as of 2026.
Japan: Voluntary manufacturer take-back programs with government incentives but no mandatory EPR.
Compliance considerations for healthcare facilities:
Hospitals must comply with medical waste disposal regulations regardless of recycling program participation. Key requirements include:
- Proper segregation of contaminated vs. non-contaminated gloves
- Documentation of waste handling procedures
- Staff training on waste classification
- Manifests for regulated medical waste transportation
- Record retention (typically 3-5 years)
Regulatory trends:
The regulatory landscape is moving toward mandatory EPR, driven by:
- Growing recognition of single-use medical device waste as environmental problem
- Success of EPR programs for other product categories (electronics, packaging, batteries)
- Healthcare sector sustainability commitments
- Pressure from environmental advocacy groups
Experts predict that by 2030, most developed countries will have some form of EPR regulation for medical gloves, though implementation timelines and specific requirements will vary significantly by jurisdiction.
A common mistake is assuming that recycling programs automatically ensure regulatory compliance. Facilities must still meet all medical waste disposal requirements even when participating in recycling programs. Recycling is an additional activity, not a replacement for proper medical waste management.
Frequently Asked Questions
Can I recycle nitrile gloves at home in my curbside recycling bin?
No, nitrile gloves cannot go in curbside recycling bins. They require specialized collection and processing through dedicated programs. Placing them in regular recycling contaminates other recyclables and they’ll be sorted out and sent to landfills anyway.
How long do nitrile gloves take to decompose in landfills?
Conventional nitrile gloves take approximately 100-200 years to fully decompose in landfills. They break down into microplastics that persist in the environment indefinitely. Biodegradable nitrile gloves decompose faster (5-10 years in industrial composting) but still require decades in typical landfill conditions.
Are powder-free nitrile gloves easier to recycle than powdered gloves?
Powder-free gloves are slightly easier to recycle because they don’t require removal of cornstarch powder during processing. However, most recycling programs accept both types. The contamination risk from medical use is a much bigger factor than whether gloves are powdered.
Can veterinary clinics participate in nitrile glove recycling programs?
Yes, veterinary clinics can participate if they meet volume minimums and contamination protocols. Gloves from administrative areas and routine wellness exams typically qualify, while gloves from surgical procedures or infectious disease treatment must be excluded, similar to human healthcare facilities.
Do recycled nitrile gloves contain harmful chemicals?
Properly processed recycled nitrile is safe for its intended applications (playground surfaces, athletic tracks, mats). Recycling facilities test for contamination and harmful substances. However, recycled nitrile should not be used for food contact or medical applications due to potential contamination concerns.
How much CO2 is saved by recycling nitrile gloves instead of landfilling them?
Recycling nitrile gloves saves approximately 0.8-1.2 kg of CO2 equivalent per kilogram of gloves compared to landfill disposal. This includes avoided methane emissions from landfills and reduced virgin material production. A hospital recycling 10,000 pounds annually saves roughly 4-5 metric tons of CO2 equivalent.
Can I start a glove recycling program if my hospital uses multiple glove brands?
Yes, most recycling programs accept multiple brands of nitrile gloves. The material composition is similar across brands, making mixed-brand recycling feasible. However, verify with your specific recycling partner as some manufacturer take-back programs only accept their own brands.
What happens if contaminated gloves accidentally get into the recycling bin?
Contaminated gloves can disqualify an entire batch of collected material (typically 500-1,000 pounds). The recycling partner may reject the shipment, requiring disposal as medical waste at higher cost. Repeated contamination incidents can result in program termination. This is why strict protocols and staff training are critical.
Are there tax benefits for hospitals that implement glove recycling programs?
Some states offer tax credits or deductions for waste reduction programs, but specific benefits vary by jurisdiction. More commonly, hospitals benefit from reduced waste disposal fees and improved sustainability scores that can affect reimbursement under value-based payment models. Consult with your tax advisor about local incentives.
How do I convince hospital leadership to invest in glove recycling when it costs more?
Focus on non-financial benefits: sustainability reporting requirements, competitive positioning, staff and patient satisfaction, and potential regulatory preparation. Quantify total costs including staff time and storage, not just per-pound fees. Explore grants and EPR programs that reduce net costs. Start with a small pilot to demonstrate feasibility before requesting full-scale investment.
Can nitrile gloves be recycled multiple times or just once?
Nitrile gloves can theoretically be recycled 2-3 times, but each cycle degrades material properties. In practice, most recycled nitrile becomes lower-grade products that aren’t recycled again. The recycling process is “downcycling” rather than true circular recycling.
What’s the difference between biodegradable and recyclable nitrile gloves?
Biodegradable gloves are designed to break down faster in landfills or composting facilities but still take years to decompose. Recyclable gloves are conventional nitrile that can be processed into new products through mechanical or chemical recycling. Biodegradable gloves typically cannot be recycled, and recyclable gloves don’t biodegrade faster than conventional gloves.
Conclusion
Nitrile Glove Waste Reduction Strategies: Extended Producer Responsibility and Hospital Recycling Programs represent practical approaches to addressing the millions of tons of single-use glove waste generated annually by healthcare facilities. While technical feasibility has been proven, widespread adoption faces barriers including contamination concerns, higher costs compared to landfill disposal, limited infrastructure availability, and lack of regulatory requirements in most jurisdictions.
Extended Producer Responsibility frameworks in the European Union are demonstrating that shifting waste management costs and responsibilities to manufacturers can create the financial incentives and infrastructure needed for effective recycling programs. France and Germany’s EPR regulations are driving manufacturer investment in take-back programs and recyclable product design, with EU-wide standards expected by 2027-2028.
Hospital recycling programs, though operationally complex, can successfully divert 40-60% of glove waste from landfills when implemented with strict contamination protocols, comprehensive staff training, and adequate infrastructure. Programs work best in large facilities with dedicated sustainability staff and in regions with established recycling partners. Small clinics face higher per-unit costs but can achieve viability through regional consortiums and grant funding.
The economics of glove recycling remain challenging, with recycling typically costing $0.15-0.30 per pound compared to $0.08-0.12 for landfill disposal. However, total waste management costs can decrease when accounting for reduced general waste pickups, EPR rebates, and sustainability grants. Facilities must calculate total lifecycle costs rather than focusing solely on per-pound disposal fees.
Actionable next steps for healthcare facilities:
Conduct a waste audit to quantify your potentially recyclable glove volumes and identify high-volume, low-contamination collection areas.
Research available programs by contacting major manufacturers about take-back programs and investigating regional recycling companies serving your area.
Calculate total costs including staff time, infrastructure, storage, and collection fees, then compare against current disposal costs and potential grants or EPR rebates.
Start small with a pilot program in 2-3 departments (administrative areas, food service, outpatient clinics) before expanding facility-wide.
Invest in training with initial sessions plus quarterly refreshers to maintain low contamination rates and high participation.
Track metrics including pounds recycled, contamination rates, costs, and participation rates to demonstrate value and identify improvement opportunities.
Explore alternatives including reusable gloves for non-clinical applications, appropriate use protocols to reduce unnecessary glove consumption, and thinner gloves where adequate for clinical needs.
Engage with policy by supporting EPR legislation in your jurisdiction and participating in industry discussions about waste reduction standards.
For facilities in regions without recycling infrastructure, focus on waste reduction through appropriate use protocols and right-sizing glove selection. These strategies can reduce consumption by 15-30% without requiring recycling partnerships.
The future of nitrile glove waste management will likely involve mandatory EPR in most developed countries, expanded recycling infrastructure, improved biodegradable materials, and greater emphasis on waste reduction rather than just end-of-life management. Healthcare facilities that implement programs now will be better positioned for future regulatory requirements while demonstrating environmental leadership.
Understanding the fundamentals of nitrile gloves and their applications helps facilities make informed decisions about which gloves to purchase, how to use them appropriately, and which waste reduction strategies will be most effective for their specific circumstances.
SEO Meta Title: Nitrile Glove Waste Reduction: EPR & Hospital Recycling